
Table of Contents
Name of the heading 1
Why Nursing's Most Persistent Pipeline Constraints (Capacity, Readiness, and Retention) Require a Strategy, Not Just a Platform
Nursing programs turned away more than 60,000 qualified applicants last year. Not because students weren't interested, but because the infrastructure to teach them wasn't there. At the other end of the pipeline, roughly 30% of newly licensed nurses leave bedside roles within their first year.
That's a system problem, not an education problem. And it won't be solved by hiring faster, competing harder for clinical placements, or asking faculty to do more with less. Those levers have been pulled. They're constrained by market forces that no single institution controls.
What's changing is how senior academic and workforce leaders are thinking about virtual reality simulation. The programs making measurable progress aren't treating VR as a classroom tool. They're treating it as workforce infrastructure, a strategic asset that scales across the full continuum of nursing development, from pre-licensure through transition to practice through long-term retention.
Here's what that shift looks like in practice.
Download the VR Workforce Guide
1- Start your table with the syntax {start-table}
2 - Add an H3 Heading to create a new column (this will be the column title)
3 - List cells as bullet points in a List element
4 - End your table with the syntax {end-table}
Pre-Licensure: Unlocking Capacity Without Unlocking Costs
Traditional simulation runs at roughly a 1:8 faculty-to-student ratio. A VR-enabled model lets one or two instructors supervise dozens of learners simultaneously. The National Council of State Boards of Nursing has endorsed this approach, and 22 states now authorize clinical hour substitution up to 50%.
The University of Manitoba used VR to expand its BSN program by 50% when hospital partners couldn't accommodate more clinical rotations. NHL Stenden University in the Netherlands became the only applied university in the country to grow nursing enrollment, enabled by VR-extended hospital partnerships. These are capacity gains that hiring alone could not have produced.
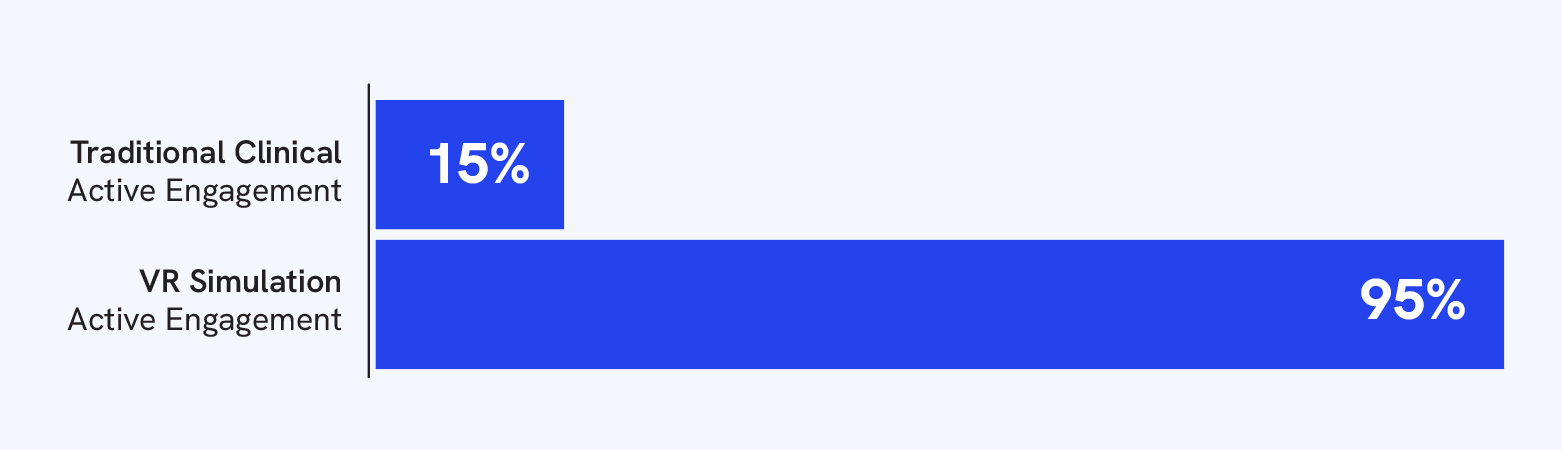
The quality signal is just as clear. During a period when national NCLEX pass rates dropped 6.5%, VR-enabled programs rose 0.87 points. Active learner engagement in traditional hospital clinicals runs around 15%, and in VR-based specialty training, it rises to 95%. Every learner practices rare scenarios regardless of what situations presented on clinical day.

Transition to Practice: Closing the Readiness Gap
Capacity alone doesn't build a workforce. Graduates have to make it through orientation and stay.
This is where the pipeline is quietly breaking. New nurses aren't leaving purely because of burnout. They're leaving because they don't feel competent. They finish school with limited procedural exposure, hit orientation, and discover that the shortage itself means they won't receive the extended mentoring previous cohorts did. The preceptors training them are often stretched just as thin.
VR-based transition-to-practice and nurse residency programs address this directly. NYU Langone Health uses VR in its nurse residency programs to reduce new graduate anxiety around emergency situations through practice with patient deterioration scenarios. Monarch Healthcare Management standardizes VR training across 22 sites to ensure consistent new nurse competency development. The University of West Florida uses VR to bridge the knowledge-practice gap, building confidence before clinical practice rather than during it.
The outcomes are measurable. VR training delivers roughly 40% cost savings versus physical simulation. Decision-making accuracy improves by 16.7%, patient safety events drop by 52%, and nurses who train with VR show 83% professional competence and 75% lower clinical anxiety.
Retention: The ROI Case That Gets Executive Attention
Replacing a single registered nurse costs between $56,300 and $61,110. For a health system losing 15 to 20 new graduates annually, that's a seven-figure exposure. The representative case in our full guide models $1.16 million in annual turnover cost.
Health system partners are already doing this math. Systems that fund consortium VR implementations with regional nursing programs understand the direct line from training investment to retention outcomes. Preceptors who aren't re-teaching basic procedures have time to mentor. New graduates who arrive already competent in fundamental skills hold that competence two months post-training. The turnover math starts to bend.
This is what it means to treat VR as workforce infrastructure rather than edtech: the metrics on the scoreboard are graduates produced, NCLEX trends, first-year retention, time-to-competency, and preceptor burden, all the same metrics state workforce boards and accreditors already track.
{start-table}
VR Infrastructure
- First-Year Cost: ~$75K
- Cost per Additional Student: $1K-$1.5K
- Implementation Time: 1-3 months
- Control: Internal
Traditional Capacity Expansion
- Annual Faculty Cost: $500K+
- Cost per Additional Student: $10K+
- Implementation Time: 6-12 months
- Dependencies: External
{end-table}
The Intentionality Premium
Here's the part that doesn't get said often enough: VR alone does not produce any of these outcomes.
Programs that plug in headsets without faculty buy-in, curricular alignment, or structured debriefing see the headsets go unused. The institutions producing the capacity gains, NCLEX improvements, and retention outcomes all share the same implementation pattern:
- A dedicated faculty champion
- Scenario design mapped to AACN Essentials and the NCSBN Clinical Judgment Measurement Model
- Alignment with INACSL Standards of Best Practice
- Debriefing treated as the core learning event rather than an afterthought
Intentional design is the difference between a capital expense and a workforce strategy. It's also why the strategic conversation has to move past "should we invest in VR" to "how do we implement VR so it actually changes our workforce metrics."
What Comes Next
The competitive dynamics are already visible. Programs investing in VR infrastructure now are expanding enrollment by 25–50%. Programs delaying investment remain constrained by the same clinical placement and faculty shortages that have existed for years. That capacity advantage, once established, doesn't redistribute easily.
For senior academic and workforce leaders, the strategic question isn't whether VR becomes standard workforce infrastructure, comparable to skills labs or simulation centers. It's which institutions will have built capacity when regional demand peaks further, and whose graduates will fill those roles.
Our full strategic guide, How Virtual Reality Strengthens the Nursing Workforce Pipeline, unpacks the evidence base, ROI framework, institutional case studies, and a six-step action plan for senior academic and workforce leaders ready to move.

FAQs
Heading 1
Heading 2
Heading 3
Heading 4
Heading 5
Heading 6
Lorem ipsum dolor sit amet, consectetur adipiscing elit, sed do eiusmod tempor incididunt ut labore et dolore magna aliqua. Ut enim ad minim veniam, quis nostrud exercitation ullamco laboris nisi ut aliquip ex ea commodo consequat. Duis aute irure dolor in reprehenderit in voluptate velit esse cillum dolore eu fugiat nulla pariatur.
Block quote
Ordered list
- Item 1
- Item 2
- Item 3
Unordered list
- Item A
- Item B
- Item C
Bold text
Emphasis
Superscript
Subscript
It means using VR simulation as a strategic asset across the full continuum of nursing development, pre-licensure capacity, transition to practice, and long-term retention, rather than as a standalone classroom tool. With 60,000+ qualified applicants turned away last year and 30% of new nurses leaving bedside roles within their first year, the infrastructure gap is too significant for incremental solutions.
By replacing hard-to-scale clinical placements with VR simulation, programs can teach more students with fewer faculty and less reliance on hospital partners. NCSBN regulatory guidance confirms that high-quality simulation can substitute for a defined portion of traditional clinical hours, and 22 states now authorize substitution up to 50%. One faculty member can supervise dozens of learners simultaneously, compared to roughly 1:8 in traditional simulation.
Yes. Nurses who train with VR show 83% higher professional competence and 75% lower clinical anxiety, two factors directly tied to first-year attrition. For health systems where replacing a single RN costs between $56,300 and $61,110, losing 15–20 new graduates annually is a seven-figure exposure that VR-based residency programs are built to address.


Tracy's work sits at the intersection of clinical learning and product strategy helping the field understand not just what VR simulation can do, but why it matters right now. She is passionate about connecting innovation with real-world impact and championing nurses at the forefront of one of healthcare's most critical transformations.
Explore more
VR Is Nursing Workforce Infrastructure, Not Just Educational Technology
Here's what it looks like when programs invest in VR as workforce infrastructure and expand enrollment by 25–50%.

How to Write Grant Applications That Actually Get Funded for VR Nursing Education
Learn how to position VR as workforce infrastructure with ready-to-use grant language for nursing education funding.
.jpg)
Step Into VR Simulation: A Nurse-Led Guide to Implementation
A step-by-step nurse-led guide to implementing VR in nursing education, with practical strategies, faculty tips, and interactive workbook activities.

